Living with Prostate Cancer
If feasible, choose a doctor specializing not just in cancer but also in the specifics of your form of prostate cancer. For example, if you’ve just been diagnosed with prostate cancer, talk to your diagnosing doctor first. They may be an expert in the subject or recommend you to someone else.
Other things to think about while choosing a doctor are: 
- Does your health insurance cover it
- Are they analytical
- Compassionate
- Does your “bedside manner” match your personality
- Do they appear eager to include you as a participant in this process
Don’t be hesitant to obtain a second or even third opinion. Random advice, such as “surgery is the best,” “radiation is the best,” or “take this herb and your cancer will be healed,” should be avoided. Instead, use data from credible sources and those your doctor advises for the most up-to-date information.
Once you’ve committed, trust is essential, but you should continue to be your advocate by asking questions, conducting research, and remaining interested.
Detect it, Treat it, Defeat it!

Early Warning Signs of Prostate Cancer
The World Health Organization stated that prostate malignancy is one of the deadliest ailments for men. In addition, the indications of prostate malignant growth may shift starting with a few symptoms and signs and then after different illnesses, which Prostate Cancer may be difficult to diagnose. This is why it is imperative to identify and not overlook these issues.
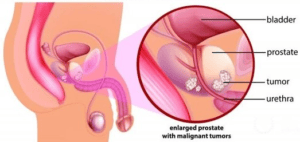
Cancer and an enlarged prostate cause similar symptoms, so it’s essential to understand the differences. Unfortunately, symptoms of prostate cancer usually don’t appear until the disease has advanced. So, while regular screenings are the best way to catch it, here are some red flags that it’s time to see a doctor.
- A few symptoms point to prostate problems, both benign and cancerous. To be safe, inform your doctor if you have any of the following issues.
- Peeing problems: A weak stream, trouble getting the flow started, or an urgent need to go (especially at night) are signs that your prostate is enlarged from BPH or cancer.
- Blood in your urine This symptom could indicate a urinary tract infection, but it’s worth checking out.
- Pain or discomfort when you pee or sit may also be due to an infection, but see your doctor to ensure. Pain in your back, chest, or hips is a sign of more advanced cancer that has spread to the bones.
- Erectile dysfunction: Although this problem plagues some men naturally as they age, prostate cancer also can interfere with your ability to get an erection.
- Painful ejaculation Less semen than usual during ejaculation and blood in your semen are other prostate cancer warning signs.
- Late-stage prostate cancer can cause bone pain, weight loss, and back pain, along with urinary symptoms. “Again, these are pretty generic symptoms that can be hard to recognize and represent something different most of the time.
Genetics/Genomics Screening
Up to age 76, prostate-specific antigen (PSA) screening was associated with a lower all-cause mortality rate, except for men with cognitive dysfunction. Categories of genetic-based biomarkers include common germline single-nucleotide polymorphisms, rare germline genetic mutations (e.g., BRCA1/2, HOXB13), and somatic (tumor) gene expression panels (e.g., Oncotype Dx®, Decipher®). For PC risk assessment, a polygenic risk score incorporating 269 PC risk single-nucleotide polymorphisms is more accurate for assessing risk for PC than the family history recommended by National Comprehensive Cancer Network® guidelines. Most single-nucleotide polymorphisms work across races, and 50% of aggressive tumors occur in men in the top 20th percentile of the polygenic risk score. A study reported that polygenic risk score is associated with conversion from active surveillance (AS) to treatment. Rare highly penetrant germline variants (e.g., BRCA2, ATM) also are associated with risk. Together, the familiar and rare variants lead to more precise estimates of the lifetime risk of PC. Plasma cell-free DNA may become essential for managing patients with advanced PC, as it is prognostic for overall survival, selecting therapy, and response to treatment. It may be more helpful than repeated biopsies.
Health Disparities
Outside the equal-access Veterans Administration (VA) system, Black men were more likely to present with metastatic disease. They had correspondingly higher PC mortality rates, but the VA system did not observe these differences. However, VA studies of men who were potential candidates for AS reported that Black patients were more likely to have an intermediate-risk disease, less likely to receive conservative management, and more likely to receive definitive therapy within five years. Most of the racial disparities appear to be due to sociodemographic factors. Among those managed with AS, Black men were reported to have more frequent disease reclassification, progression, and definitive treatment but not more metastasis or higher PC-specific mortality. A multi-institutional AS study outside the VA system found no association of race with conversion to treatment. Thus, AS appears comparably safe for Black and White men. PSA velocity was reported to be associated with Gleason-grade progression and metastases, but the thresholds were lower for Black men.
Biopsy
Transperineal prostate biopsy is being increasingly adopted (in a third of urologists recently polled) to reduce the risk of sepsis (even without antibiotics) and, with fusion guidance, to provide an improved sampling of the apical and anterior regions of the prostate. The challenges of transperineal biopsy are patient comfort, the need for a template, increased time, overhead, and difficulties with insurance coverage. In addition, a transperineal biopsy involves a substantial learning curve for where and how to achieve local anesthesia, which takes practice and experience. Currently, about half are performed under intravenous sedation.
Lymph Node Metastases
Several studies failed to find clear benefits from extended pelvic lymph node dissection, while others demonstrated a use associated with radiotherapy to involved pelvic nodes (see Radiotherapy section below). With the emergence of prostate-specific membrane antigen (PSMA)-positron emission tomography (PET) imaging, the management of nodal metastases may become an increasingly important issue.
Imaging
Magnetic Resonance Imaging (MRI): MRI increases the accuracy of diagnosing PC but does not identify which men need treatment. Serial prostate MRI alone in patients on AS is not sufficiently accurate to rule out or rule in tumor reclassification or progression. Biparametric MRI protocols are quicker, less expensive, and more accurate than those using ultrasound plus PSA alone. A study of men who never had a biopsy compared standard systematic ultrasound versus MRI-targeted biopsy taking only 2–3 cores from the MRI region of concern found that the targeted biopsy alone was non-inferior to systematic biopsies. Over a third of MRI patients avoided a biopsy, and there were 50% fewer low-grade diagnoses. Other studies have shown that adding systematic biopsies is of value and should remain part of the process. It is not unusual to find significant cancers in the systematic cores, even in areas with a normal MRI appearance. MRI is not sufficiently accurate to substitute for surveillance biopsies but is helpful overall. Patients with high Prostate Imaging–Reporting and Data System (PI-RADS™) lesions and negative initial biopsies should have repeat MRI scans. If the high PI-RADS abnormalities persist, undergo a repeat biopsy (including peri-lesion biopsies), as nearly two-thirds of these may reveal cancer. Positive target biopsies should be counted as only one positive core (i.e., the most extensively involved core).
PSMA PET: Because of their high sensitivity and specificity, the PSMA PET scans (gallium and fluorine) may significantly impact patient management. One study reported that half of the patients with positive PSMA PET scans had a serum PSA <0.2 ng/uL.26 The most accurate platform would include the PSMA PET with MRI (rather than computerized tomography), which increases the sensitivity for high-risk tumors.
Radiation Therapy
In the FLAME trial, men receiving higher doses of MRI-defined tumor nodules had a twofold reduction in biochemical failure and no additional toxicity. In the POP-RT study, treating pelvic lymph nodes improved biochemical control and distant-metastasis-free survival at the cost of a mild increase in late genitourinary toxicity. In the PROSINT trial, men receiving treatment in a single fraction or five fractions had similar biochemical outcomes and toxicity. In the postoperative setting, three randomized studies evaluated the role of adjuvant radiation in men with high-risk disease after prostatectomy. The largest of these (RADICALS) and a meta-analysis showed that early salvage therapy, when needed, did not compromise outcomes and spared a significant proportion of men from unnecessary treatment. The SAKK 09/10 study demonstrated that dose escalation from 64 to 70 Gy did not improve biochemical outcomes and added toxicity. The EMPIRE-1 research suggested that fluciclovine PET improved biochemical effects when used to select men and plan postoperative radiation compared to conventional imaging. In oligo-recurrence in regional lymph nodes, the GETUG07 study demonstrated ∼50% biochemical control at three years of follow-up with pelvic radiation and six months of hormonal therapy (ADT). In the setting of metastatic disease, a secondary analysis of the STAMPEDE trial suggested that survival is improved after prostate radiation, particularly in men with only lymph nodes or three or fewer bony metastases.
Advanced Disease
Men with locally advanced disease account for ∼15% of patients with newly diagnosed PC and have relatively poor cancer-specific mortality. In a prospective neo-adjuvant trial for patients with high-risk disease, either six months of ADT with apalutamide + abiraterone/prednisone + leuprolide vs. abiraterone/prednisone + leuprolide, adding the third agent didn’t make a difference. Still, there was a remarkable 20% complete response or minimal residual disease rate. A meta-analysis of neo-adjuvant trials found that 60% of patients were without biochemical recurrence after three years. In patients who achieve a complete response/minimal residual disease, there is a significant difference in the recurrence rate (8% vs. 50%). Thus, a robust response to ADT is a good indicator of outcomes in the neoadjuvant setting. Oral relugolix is a luteinizing hormone-releasing hormone antagonist. A trial of relugolix vs. leuprolide showed that relugolix achieved superior testosterone suppression and occurred faster, whereas the cardiovascular side effects were lower. A meta-analysis also showed that cardiovascular events are more frequent with the luteinizing hormone-releasing hormone agonists than with the antagonists. However, the high cost of relugolix limits its adoption. Enzalutamide is superior to bicalutamide in Black patients, but bicalutamide can be safely used to prevent testosterone flare-ups in Black patients. For castrate-sensitive PC, abiraterone and apalutamide have the best results for survival, and these agents do not seem to cause a cognitive decline. Zoledronic acid and denosumab are approved for preventing or delaying skeletal-related events. Zoledronic acid may compromise renal function, whereas denosumab may cause hypocalcemia. Osteonecrosis of the jaw occurs at approximately the same rate with both agents. Denosumab is far more expensive. These agents improve survival in patients with castrate-resistant disease and reduce skeletal-related events. They should be used in all patients with bone metastases who are castration-resistant.
In a study of olaparib (a PARP inhibitor used in patients with homologous DNA repair deficiency mutations such as BRCA1/2) vs. abiraterone/enzalutamide (crossover), in which 30% of patients had some pathogenic mutation, there was a significant improvement in overall survival, especially in patients with BRCA mutations. Another study reported that cabazitaxel was advantageous for patients with a mutation other than BRCA. In a trial comparing lutetium-177-PSMA-617 (a radioligand therapy targeting PSMA) with standard care using ADT in patients with PSMA highly expressed on their metastases, there was a significant survival advantage for the lutetium arm. Unfortunately, this radioligand treatment is not yet U.S. Food and Drug Administration-approved. Immunotherapy has been disappointing for PC. However, a study of nivolumab plus ipilimumab for metastatic castrate-resistant PC showed a 25% response rate in the pre-chemotherapy setting with a better response rate in patients whose tumors had a high mutational burden.48 This regimen was quite toxic.
References:
William J. Catalona, MD; Douglas M. Dahl, MD; Stanley L. Liauw, MD; Stacy Loeb, MD, MSc, Ph.D. (hon); Robert B. Nadler, MD; Russell Z. Szmulewitz, MD
Perdana NR, Mochtar CA, Umbas R, Hamid AR. The Risk Factors of Prostate Cancer and Its Prevention: A Literature Review. Acta Med Indones. 2016